One of the biggest mistakes in dentistry is believing that quality depends only on the dentist’s technical level.
As if a skilled clinician could produce quality always, in every condition, with every agenda, with every assistant, with every patient, with every economic pressure, with every interruption, and with every mental load.
But this is not true.
Quality is not only a property of the hand.
Quality is a property of the system in which that hand works.
A dentist may have competence, culture, experience, vision, manual ability, and clinical sensitivity.
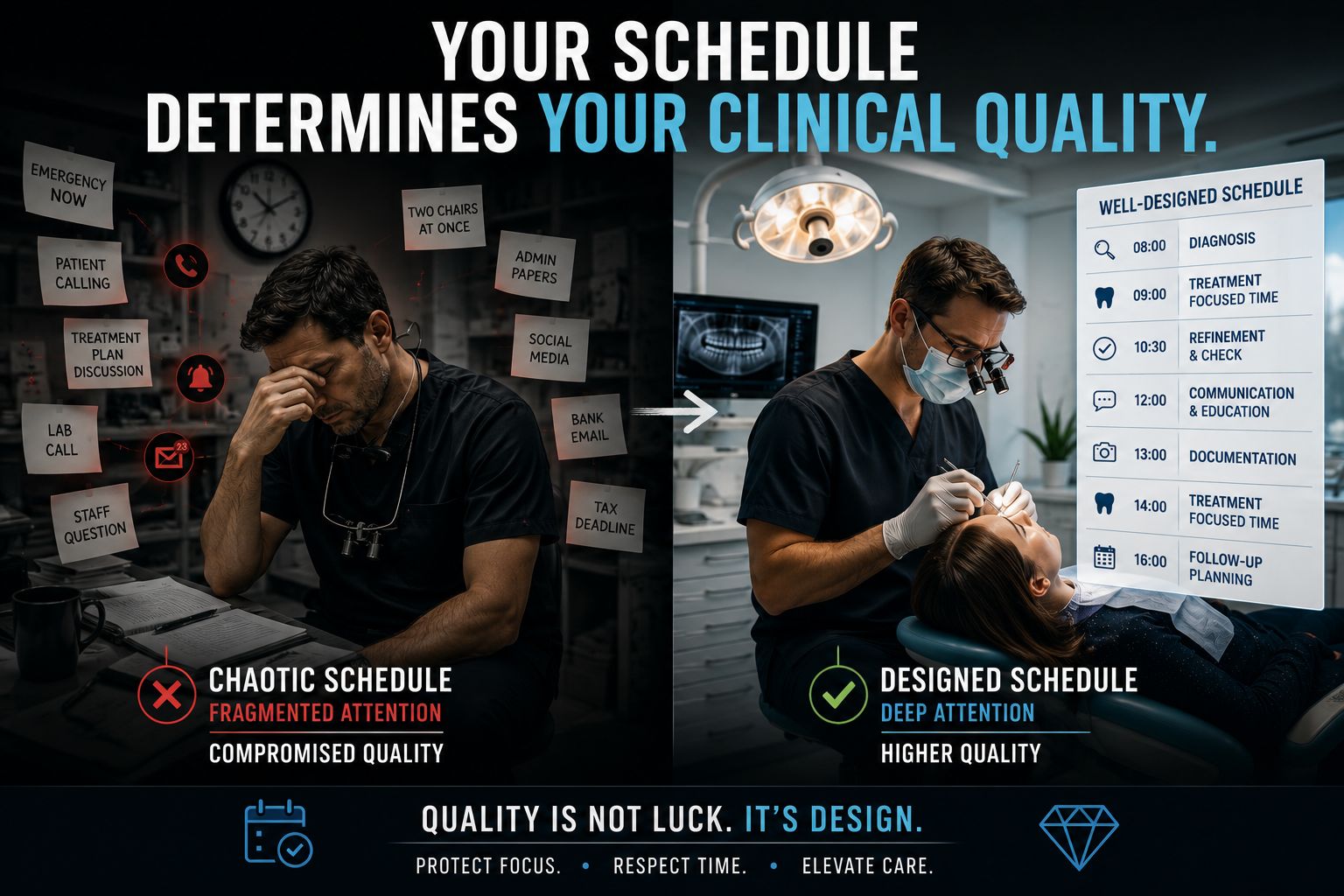
But if he works constantly late, if he is interrupted, if he has to move between two chairs, if he enters the operatory already mentally full of administrative problems, if he has no time to take pictures, refine, check, explain, evaluate, or follow up, that competence does not disappear.
It simply cannot fully appear.
Many dentists are not less skilled than they think.
They are simply working in conditions where their skill cannot express itself.
The same operator in different context will soon perform in different ways.
This is the uncomfortable truth.
A lot of mediocre dentistry is not produced by mediocre dentists.
It is produced by mediocre working conditions.
Too many patients.
Too little time.
Too many interruptions.
Undefined roles.
Assistants not properly prepared.
Diagnoses made too quickly.
Treatment plans discussed between a cavity and a crown preparation.
Emergencies added into days that were already impossible.
The owner running from the operatory to the reception desk, from the patient to the accountant, from the clinical problem to the bank, from the team conflict to the marketing decision.
And then we wonder why quality does not happen.
But quality is not an heroic act.
Quality is the predictable result of an environment that makes it possible.
A beautiful posterior composite, a stable crown margin, a biologically respectful preparation, a correct periodontal diagnosis, a well-managed provisional, a precise adhesive procedure: none of these things depends only on knowledge.
They also depend on space.
Mental space.
Technical space.
Temporal space.
A good restoration does not need only composite, adhesive, matrices and instruments.
It needs the dentist to remain inside the case long enough to see what is easy to miss.
The small detail.
The hidden margin.
The bleeding point.
The occlusal interference.
The soft tissue reaction.
The patient’s doubt.
The assistant’s uncertainty.
The part of the procedure that still needs one more minute, one more check, one more look.
Quality often does not die in dramatic mistakes.
It dies in small compromises repeated every day.
Five minutes removed from isolation.
Three minutes removed from finishing.
One occlusal check done too quickly.
One picture not taken.
One explanation shortened.
One follow-up never scheduled.
Each compromise looks small.
But together they become a culture.
And in a dental office, culture is often created by the agenda.
This is why the schedule is not an administrative tool.
The schedule is a clinical instrument.
We usually treat the agenda as a grid to fill.
A container for production.
A Tetris of patients, emergencies, hygiene appointments, checks, cementations, impressions, consultations, “doctor, just five minutes.”
But the agenda is not neutral.
The agenda decides before us how good we are allowed to be that day.
It decides whether we will enter the room already late.
It decides whether diagnosis will be real or superficial.
It decides whether we will check the margin or simply move on.
It decides whether we will listen to the patient or mentally pass through him to reach the next one.
It decides whether a procedure will be performed with presence or with divided attention.
An agenda designed only around production creates reactive dentistry.
An agenda designed around quality creates the conditions in which production can become a consequence.
The point is not to work slowly.
The point is to give each procedure the biological, technical, and mental time it requires.
A complex diagnosis cannot be treated like a quick check.
A first visit cannot be just a corridor toward the treatment plan and its price.
An adhesive case cannot be done with the mind divided between the rubber dam and the patient in the second chair.
A rehabilitation cannot be inserted between two emergencies and still pretend to be a thoughtful act.
Dentistry requires attention.
Not generic attention.
Deep attention.
And deep attention is fragile.
It cannot survive constant interruptions, undefined roles, last-minute changes, emotional pressure, commercial conversations, clinical uncertainty, and an owner who has become the nervous system of the entire practice.
Because this is another uncomfortable truth: in a small dental ecosystem, being the owner is often the worst possible condition for producing clinical quality.
The owner is not only a dentist.
He is often the commercial manager, the marketing director, the human resources department, the production manager, the research and development department, the motivator, the controller of other departments, the person who deals with taxes, banks, collaborators, patients, conflicts, complaints, and all the problems nobody else knows how to solve.
Being the owner is difficult because the owner does not have one job.
He has all the jobs that are not clearly assigned to someone else.
And when roles are not defined, everything returns to the owner.
Every doubt.
Every interruption.
Every conflict.
Every decision.
Every small organizational weakness.
At that point, the practice is no longer an organization.
It becomes an extension of the owner’s overloaded nervous system.
And when the owner does not function, very often the office does not function either.
If the owner is confused, the practice becomes confused.
If the owner is reactive, the practice becomes reactive.
If the owner works always in emergency, the entire team learns that emergency is normal.
If the owner does not protect clinical focus, nobody else will.
This is why quality cannot be separated from organization.
We like to talk about materials, techniques, protocols, scanners, composites, ceramics, implants, preparation designs, bonding systems, digital workflows.
And of course all of these things matter.
But before all of that, there is a simpler and more brutal question:
Did we create the conditions to use them well?
Because a good material in a bad system becomes an average result.
A good protocol in a chaotic agenda becomes an intention.
A good dentist in a fragmented day becomes a reduced version of himself.
Clinical quality is not the product of skill in the abstract.
It is the product of protected skill.
And maybe this is one of the most important responsibilities of a dental owner: not doing everything, not controlling everything, not being everywhere, not solving every problem personally.
But designing a practice where quality has somewhere to live.
A place in the agenda.
A place in the roles.
A place in the protocols.
A place in the team culture.
A place in the mind of the clinician.
Because every practice has the quality that its agenda allows.
Not the quality the owner declares.
Not the quality the website promises.
Not the quality the dentist imagines he can offer.
The real quality is the one that survives inside the spaces the system gives it.
And if there is no space, there will be no flow.
And if there is no flow, dentistry becomes damage control.
Not because the dentist does not care.
But because caring is not enough when the system is designed to interrupt the very attention that quality requires.
Nex time you look your scheduling …stop for a while and look with attentino.
There lies what is limiting your potential.
